
Lean methodology is a quality improvement strategy with the overarching goal of using less to do more.
It’s applied across industries with its origins in manufacturing, but the core goals of lean methodology are the same: reduce waste, improve process, improve quality, increase efficiency — at all levels of an organization.
How is lean methodology used in healthcare?
Lean methodology in healthcare considers employees, customers, patients, and continuous improvement at its core.
According to NEJM catalyst journal, “Using lean principles, all members of the organization… continually strive to identify areas of waste and eliminate anything that does not add value for patients.”
Lean methodology might ring a bell to Deming’s theory for quality improvement, birthed from the manufacturing industry where efficiency and waste reduction is directly correlated to profits.
Theis methodology applies to healthcare, but with the heart of the system centering around not only profits, but people: patient satisfaction, quality of care, efficiency of processes, and employee and customer experience, which all can be improved sustainably over time.
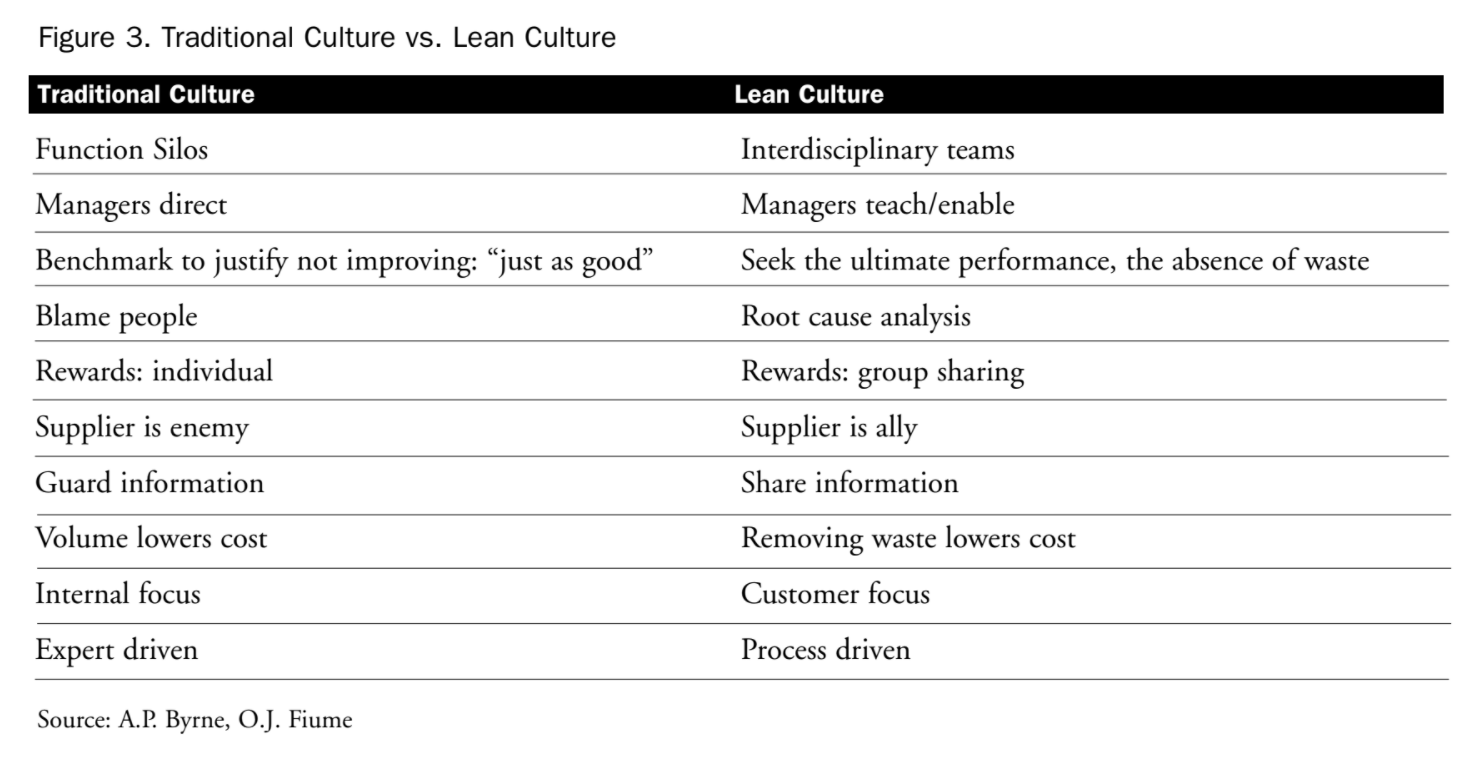
Traditional Culture vs. Lean Culture
As published in the Innovation Series: Going Lean in Health Care white paper (Womack, J. et al, 2005), the figure below shows how traditional culture and lean culture have marked differences in how team members focus, interact, and view each other and their work.
Lean Implementation in Healthcare
Higher patient satisfaction, improved quality of care, improved processes, and reduced waste in processes, procedures, and tasks.
These are just some of the major benefits that implementing a lean healthcare methodology over time can produce. As a long-term strategy, lean healthcare will create a culture for continual, sustainable improvement that benefits people as well as systems and profits.
The case study below illustrates an example of lean implementation in healthcare in practice, and the roadblocks that can occur.
A common roadblock in implementing quality change efforts is resistance to change from leadership. The evolution of innovation and psychology of change explains that teams need leadership’s buy-in and support before implementing process changes at scale. But, real-world demonstration of the effectiveness of efforts like lean methodology can help CEOs see the benefits first-hand.
That’s what happened with Martin Judd, CEO of Saints Mary and Elizabeth Medical Center in Chicago, Illinois. According to an article in Modern Healthcare Magazine, while Judd was initially resistant to participating in a Lean breakthrough event, he turned from skeptic to “enthusiastic supporter” stating that he “was floored by what they came up with… it really demonstrated the power of giving the teams the gift of time to make the work better.”
While an anecdotal example, we can also look at the facts. Teams need CEO and leadership buy-in and support to make process changes in the name of quality improvement.
Another challenge that lean implementation helps solve is getting team members involved at a micro level, thinking critically about their processes as they perform everyday work. Do processes make sense? Where can improvements be made? When issues or bottlenecks are identified, they’re ranked in order of importance; what changes will have the biggest impact with the least effort?
These are just some of the issues that lean healthcare is built to solve as a methodology that produces long-term, effective positive change.
Related articles:
PDSA Cycles for Quality Improvement
Creating Process Maps for Improvement
Sources:
- “Innovation Series: Going Lean in Health Care.” Institute for Healthcare Improvement (2005). Based on papers written by an IHI Calls to Action Series. Womack, J.; Byrne, A.; Fiume, O.; Kaplan, G.; Toussaint, J. (2005).
- https://catalyst.nejm.org/doi/full/10.1056/CAT.18.0193

Recent Comments